




TMCC Influence: Even If You Don't "Get it"
Michael J. Mullin, ATC, PTA, PRC
The Temporomandibular Cervical Chain (TMCC) is one of a few different polyarticular chains or groups of muscles in our bodies that work together to help guide movement. We have two of these chains—one on the left side of our body and one on the right. It essentially coordinates movement of the head (cranium), jaw (mandible) and neck (cervical spine) with each other AND between both sides of the body with each other.

www.integrativecoredynamics.com
For those who have taken courses through the Postural Restoration Institute®, it is discussed briefly in their primary courses, but the secondary course “Cervical Revolution” goes much more in depth about identifying, assessing and treating dysfunction in this chain. It is heavily laden with dental, maxillary-oral-facial, osteopathic and orthopaedic concepts and can be very challenging to grasp initially. While it is important information for practitioners to be aware of who utilize the PRI treatment approach, it can be hard for some to truly “get it”. There are some great sources for reviews of these courses by Zac Cupples here and here, as well as the information from the Institute here.
I thought it would be helpful to share a recent visit with a patient to demonstrate the influence this chain can have on our system, as well as how small changes can have profound affects on the rest of the body.
I have been seeing a patient for a little bit for bilateral shoulder issues--ICD9 719.41: “Pain in joint involving shoulder region”. As many people know who treat patients in physical therapy, the diagnosis in many cases can be largely irrelevant, much like the one this physician provided. Suffice to say there are no tears or arthritis. I could also go into all of his findings, but that is not the point of this.
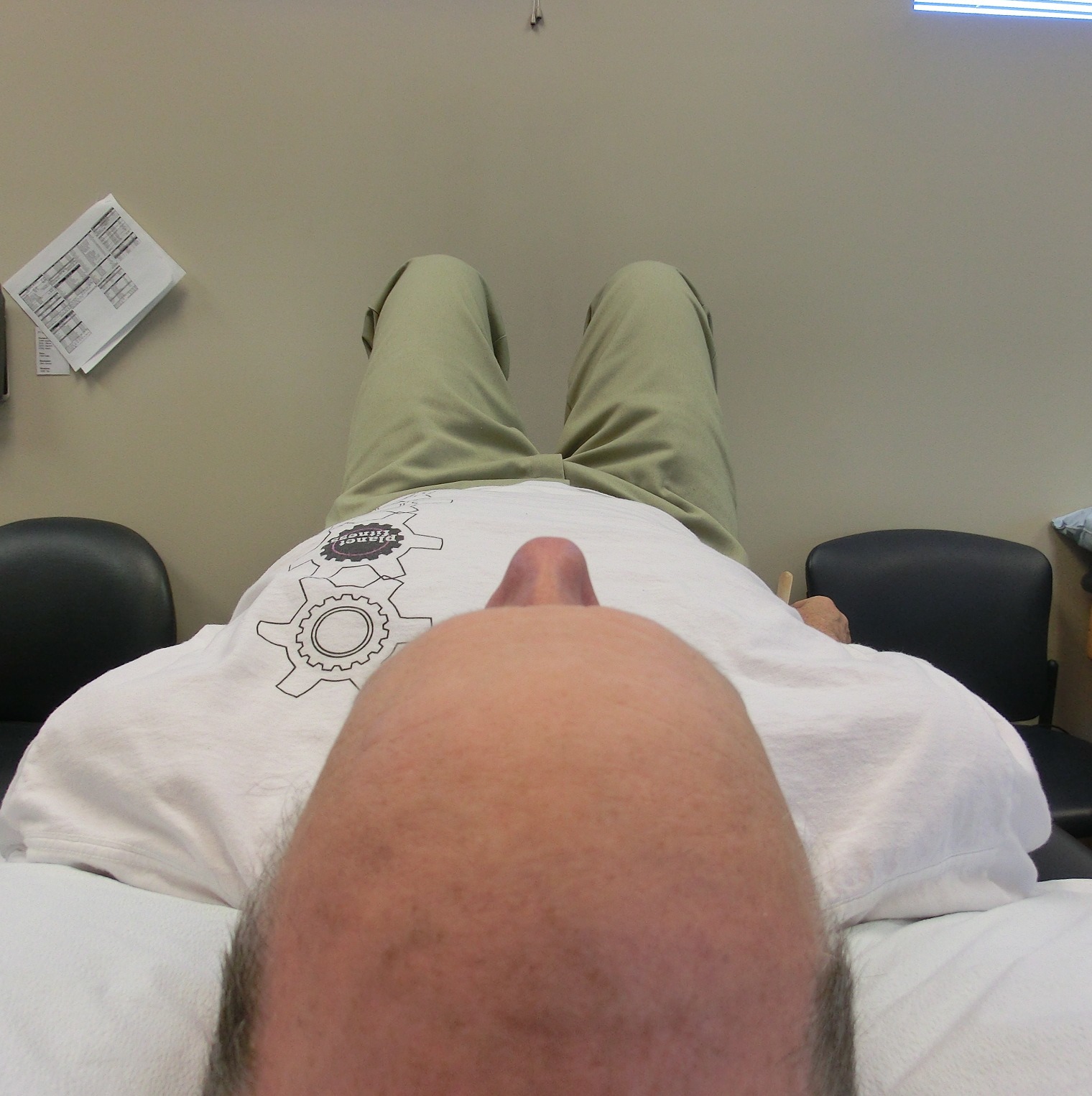
He has been making steady progress, but I also knew very early on that there was a strong top-down component which was playing a role in his symptoms and recovery--facial distortion, migrating mandible when talking, cervical sidebend, bodily orientation when talking to me, etc. It could not be addressed early on for a variety of reasons—which will be part of a future post—but today the time was right and I thought I would share a few pictures I took, which was an important part of the teaching process I used with him. I had him lie on his back on the table with tongue depressor in hand. You can actually see it in his right hand—he just has no idea what he will be doing with it :) I asked that he lie comfortably, and this is the position he assumed:

Um, a bit off center
His head is quite obviously laterally shifted to the left. We also tested his Humeral Glenoid Internal Rotation (HGIR—see picture) and used this as a before and after assessment (comparable sign) and while much better than previous weeks, it was somewhat limited bilaterally in this position as well.

HGIR Testing
I then manually moved his cranium and cervical spine to what was aligned and he said: “That’s straight?! Really?!” That picture is here:
Pictures can be deceiving. Looks straight, but he could never sustain it.
He noted (obvious) tightness and tenderness being in this position and while it looks better, his system is not able to support it. I ask him to take a few full breaths (he has been well-trained on the breath sequence I want him to be using), lift and move his head around and lie comfortably, and he ends up back here:
Default position
So I ask him to then place the tongue depressor (i.e. crude flat plane splint) between his right upper and lower teeth, take a few breaths, move his head around and lie comfortably, and it doesn’t change much at all, nor do his HGIR scores.
I then ask him to place the tongue depressor between his left top and bottom teeth, get as much balanced closure as he felt he could comfortably, and hold the tongue depressor there. (In many situations, people will know what you are asking them to do when describing this to them.) I then ask him to take a few full breaths, lift and move his head to a comfortable position and he ends up here:

His HGIR scores were completely normal in this position as well, which he could really feel. The pictures helped him see what the differences were. Two minutes of time and got ‘em—hook, line and sinker. Compliance and appreciation for what we are trying to do are now more solidly ingrained. (Full disclosure: I did nothing else to influence this head position or cue him in any way. Period.)
There is a whole more to it—and him—than this article shows, but I hope this might be a helpful visual for people who have limited to no exposure to this aspect of Postural Restoration® assessments and intervention strategies. It’s important to remember that it is a part of the treatment plan, not THE treatment plan. His HEP and weight bearing activities in particular will now be done with something like this to help create top-down closure, instructions on how to be more aware of tongue and jaw position with ADL’s (i.e. chewing, swallowing, resting position), and further aspects of the TMCC/Cervical Revolution protocol will be introduced as well.
Here’s to keeping your head on straight…..

